Accurate weight estimation is one of the most critical steps in paediatric emergency care. Almost every emergency intervention — from drug dosing and defibrillation energy to fluid resuscitation and airway selection — depends on a child’s weight. Yet in many real‑world emergencies, an exact weight is unavailable or impossible to measure quickly.
This challenge has led to the development of multiple paediatric weight estimation methods, each designed to balance speed, accuracy, and practicality. Understanding these methods, their limitations, and when to use them is essential for safe clinical practice.
This article provides an evidence‑based overview of paediatric weight estimation in emergency settings, with a focus on clinical accuracy, commonly used formulas, and best‑practice recommendations used across the UK.
Why Accurate Weight Estimation Matters in Paediatric Emergencies
Unlike adults, children require almost all medical treatments to be calculated on a weight basis. Errors in weight estimation can lead directly to medication underdosing or overdosing, incorrect defibrillation energy, and inappropriate fluid volumes.
Studies have consistently shown that medication errors are more common in paediatric emergencies, particularly during resuscitation or high‑stress situations. This risk increases when clinicians rely on mental arithmetic or estimations made under pressure.
Accurate weight estimation is therefore essential for:
- Safe drug administration
- Correct defibrillation energy
- Appropriate airway equipment selection
- Fluid resuscitation
- Reducing medication errors
For this reason, structured weight‑estimation tools are widely recommended in emergency medicine.
Common Methods of Paediatric Weight Estimation
Several methods are used internationally to estimate a child’s weight when direct measurement is not available. Each has strengths and limitations depending on the clinical context.
Age‑Based Weight Estimation
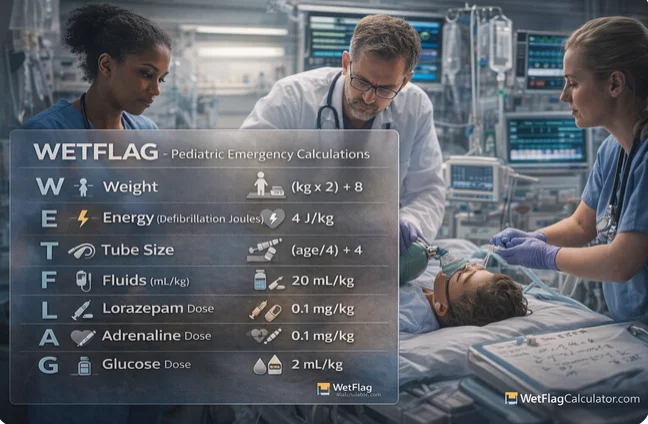
APLS Weight Formula
One of the most commonly used methods in the UK is the Advanced Paediatric Life Support (APLS) formula:
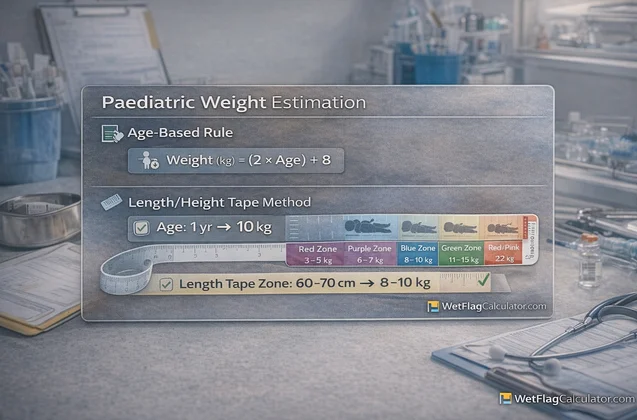
- Weight (kg) = (Age × 2) + 8
This formula is widely taught in APLS and emergency medicine training because it is quick, simple, and easy to remember.
Advantages
- Fast and easy to use
- Requires no equipment
- Suitable for emergency situations
Limitations
- Less accurate in obese or underweight children
- Less reliable in infants under 1 year
- Tends to underestimate weight in older children
Despite its limitations, the APLS formula remains widely used due to its simplicity and speed.
Length‑Based Weight Estimation
Length‑based systems, such as the Broselow tape, estimate weight using a child’s height rather than age. These tools are often more accurate than age‑based formulas, particularly in younger children.
Benefits of Length‑Based Methods
- Improved accuracy compared to age‑based formulas
- Useful in controlled environments
- Integrated drug dosing and equipment sizing
Limitations
- Requires the child to be supine and still
- Less practical in pre‑hospital or chaotic environments
- May overestimate weight in obese children
Parental or Caregiver Estimated Weight
Interestingly, studies have shown that parent‑reported weight is often more accurate than age‑based formulas, particularly when parents are confident in their estimate.
However, this method relies heavily on recall accuracy and may not be available in emergency situations where caregivers are absent or distressed.
Comparison of Weight Estimation Methods
| Method | Accuracy | Speed | Best Use Case |
| APLS formula | Moderate | Very fast | Emergency use |
| Broselow tape | High | Moderate | ED / resus room |
| Parental estimate | High (if known) | Fast | When available |
| Actual measurement | Highest | Slow | Non‑urgent care |
Digital Tools and Calculators in Clinical Practice
Digital calculators and clinical decision tools have become increasingly common in paediatric emergency care. Research shows that digital tools reduce calculation errors compared to manual methods, particularly in stressful environments.
Tools such as structured paediatric calculators allow clinicians to:
- Instantly calculate weight‑based doses
- Reduce mental arithmetic
- Improve consistency between team members
- Decrease medication errors
These tools are especially valuable when integrated into clinical workflows or used during resuscitation.
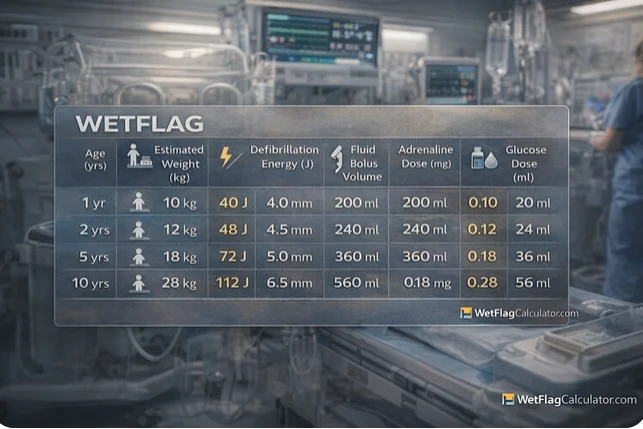
For clinicians seeking an interactive tool, an example of a structured WETFLAG Calculator is here
Clinical Best Practices for Weight Estimation
To maximise patient safety, clinicians should follow these principles:
- Use measured weight whenever available
- Use structured tools rather than mental calculation
- Reassess doses as patient condition changes
- Avoid relying on a single method in complex cases
- Follow local and national guidelines
Weight estimation should always be viewed as part of a broader clinical assessment rather than a standalone decision.
Safety Considerations and Limitations
No weight estimation method is perfect. Age‑based formulas may under‑ or over‑estimate weight depending on body composition, ethnicity, and nutritional status.
Clinicians should exercise caution in:
- Obese children
- Infants under 12 months
- Adolescents
- Children with chronic illness
Whenever possible, estimated values should be replaced with measured weight once the patient is stabilised.
Alignment with UK Clinical Guidance
Paediatric weight estimation forms part of standard emergency practice in the UK and is supported by national guidance from organisations such as:
- Resuscitation Council UK
- Advanced Paediatric Life Support (APLS)
- UK emergency medicine training bodies
These organisations emphasise structured approaches, clear communication, and the use of cognitive aids to improve patient safety.
Frequently Asked Questions
Is age‑based weight estimation accurate?
It provides a reasonable estimate but may be inaccurate in obese or underweight children. Measured weight is always preferred when available.
Is a calculator better than mental calculation?
Yes. Studies show digital tools reduce dosing errors and improve accuracy in emergency situations.
Should weight be rechecked later?
Yes. Once the child is stabilised, actual weight should be measured and all doses reviewed.
Conclusion
Paediatric weight estimation is a critical component of safe emergency care. While no single method is perfect, structured approaches such as age‑based formulas, length‑based tools, and digital calculators significantly improve accuracy and reduce risk.
Understanding the strengths and limitations of each method allows clinicians to make better decisions under pressure. When combined with clinical judgement and national guidelines, these tools play an essential role in delivering safe, effective paediatric care.
Disclaimer: This article is intended for educational purposes only and does not replace professional medical judgement, institutional protocols, or formal clinical training.
A complete guide to paediatric weight estimation in emergencies. Learn formulas, accuracy, best practices, and how clinicians safely estimate weight in children.